Aortic Valve Stenosis
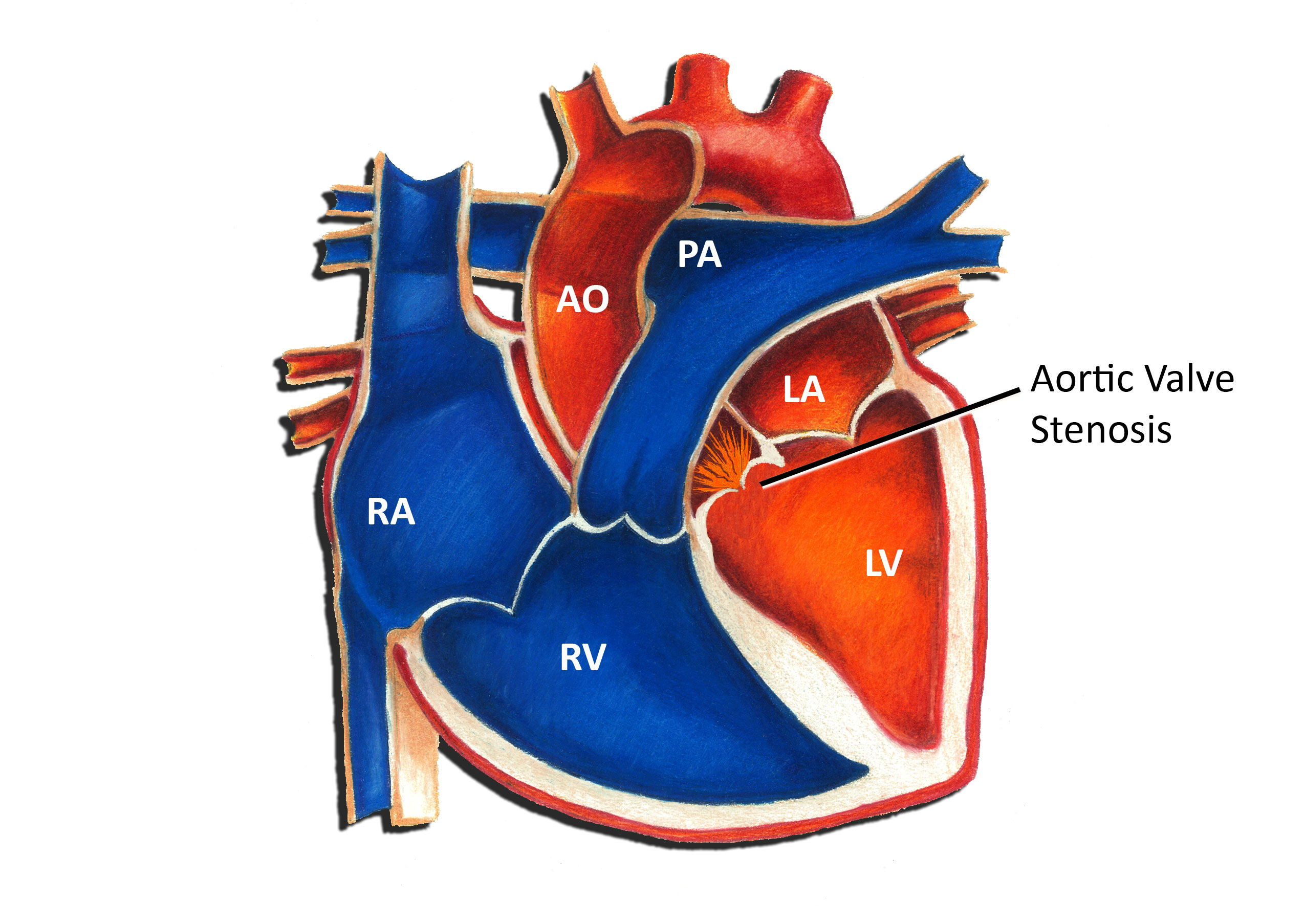
The aortic valve connects the left ventricle and the aorta. When the heart squeezes, the valve opens, allowing blood to pass from the left ventricle into the aorta. When the heart relaxes, the valve closes, preventing backflow of blood into the heart. Aortic valve stenosis refers to a condition in which the valve is abnormally narrowed. Aortic valve stenosis is a congenital heart defect, in other words, a birth defect of the heart. Congenital heart defects are the most common form of birth defects, occurring in approximately 1 in 150 individuals. Aortic valve stenosis is one of the more common congenital heart defects; the overall incidence is 0.2-0.5 per 1000. Most cases of aortic valve stenosis in young people are due to a bicuspid aortic valve. In this situation, the aortic valve has only 2 leaflets instead of the normal 3. This typically causes some degree of narrowing or leakage of the valve. In occasional instances, a bicuspid aortic valve may be an inherited or genetic problem.
Physiologically, aortic valve stenosis creates a situation in which the left ventricle must squeeze more forcefully to pump blood past the narrowed valve. The burden on the left ventricle is directly related to the degree of narrowing. A more narrowed valve results in more stress being placed on the left ventricle. In cases of mild aortic valve stenosis, there is little if any significant hemodynamic burden placed on the heart.
Symptoms from aortic valve stenosis are actually quite uncommon. The majority of patients rarely have any noticeable symptoms during infancy or childhood. Infants with severe aortic valve stenosis may develop a rapid respiratory rate or signs of impaired blood flow to the body. Occasionally older children with long standing, significant aortic valve stenosis may develop symptoms with exercise such as fatigue or even fainting.
Diagnosis of aortic valve stenosis can be made in a number of different ways. A patient with aortic valve stenosis usually comes to attention due to the presence of a heart murmur. This simply refers to the sound that blood is making as it flows past the narrowed valve. There are many other different causes of heart murmurs, including normal causes. An echocardiogram uses sound waves to visualize the intracardiac structures and is the easiest means to show the valve and degree of narrowing.
There is a wide spectrum of treatment options for a patient with aortic valve stenosis. Most patients with mild aortic valve stenosis require no specific therapy whatsoever. Unfortunately, the degree of stenosis often gradually worsens over time. Patients with mild aortic valve stenosis have a normal life-span and are free to participate in most activities without restriction.
Patients with severe or moderate to severe aortic valve stenosis require intervention to prevent long term damage to the heart. Often the initial intervention is balloon valvuloplasty through a cardiac catheterization. A catheter (a long thin tube) is placed into the heart through a blood vessel in the leg. A balloon on the end of the catheter is then used to dilate the narrowed valve. In general, the success rate for this procedure is relatively good with a low complication rate. A percentage of patients will develop some degree of leakage of the valve following the procedure, a condition termed aortic valve regurgitation.
There are a number of different surgical options for the patient with aortic valve stenosis. Options include a valvotomy (surgical opening of the valve), or replacement of the valve with a donor valve or a mechanical valve. In general, surgery for aortic valve stenosis is very successful.
Up until recently, patients with any form of heart defect, including aortic valve stenosis, were recommended to use antibiotics prior to dental work or surgery to minimize the risk of heart-related infection. However, in May 2007 the American Heart Association changed this recommendation such that now most patients with congenital heart disease, including aortic valve stenosis, no longer require this precaution.